Blast Injuries and Hyperbaric Oxygenation
Featured article. Page 7.
Acute Brain and Cardio-Respiratory Dysfunction After Blast/Blunt Injuries: The Life-Preserving Effects of Hyperbaric Oxygenation
Gennady G. Rogatsky and Avraham Mayevsky
The Mina & Everard Goodman Faculty of Life Sciences and the Leslie and Susan Gonda Multidisciplinary Brain Research Center, Bar-Ilan University, Ramat-Gan 52900, Israel
V. CONCLUSIONS
The analysis of presently available literature leads to the conclusion that in contemporary terrorist bombing blast injuries, already in the initial stages of the trauma, pronounced impairments of central hemodynamic, respiratory and CNS function can often occur. In summary, these functional impairments of vitally important organs lead to a decrease in oxygen transport in the organism, its manifestations being directly dependent on the degree of trauma severity, the level of acute cardio-respiratory dysfunction, and the blood loss volume.
The practice of the last decade shows that these impairments determine the fatal outcome for many severely injured victims already in the pre-hospitalization stage, but also in the initial hospitalization stage, during emergency and intensive care by the methods conventionally used for such cases. In cases of inadequate or late anti-hypoxic therapy, the increasing or persistent acute oxygen deficit is the basis for the subsequent acute organ and systemic damage in the post-shock period (SIRS, ARDS, multi-organ failure, etc.).
Presently, many pathogenic mechanisms of blast injury consequences, especially of its severe forms, are not known sufficiently. However, the fact of rapid development of hypoxia in these cases has been established in many researches. The existing limited number of observations has also established the beneficiary effects of hyperbaric oxygenation on the blast trauma outcomes. This result has been also confirmed in other special studies of HBO2 influence on blunt traumas of the chest and/or of the head. These results indicate that the effectiveness of HBO2 therapy in these situations can be quite high, and even life-determining.182 The mechanisms of such an effect, seen already in the very first stages of the trauma, require further investigations. However, we now have substantial grounds to consider HBO2 therapy to be a most important condition for the survival of severely injured patients in the early post-traumatic period.
Our many years of experience using HBO2 therapy in cases of severe traumas, in both clinical and laboratory settings, allow us to conclude that in the present-day circumstances, in the face of a constant and ever increasing threat of expanding terrorist actions, as well as of other means of mass destruction, there is a vital and urgent need for the restoration and development of that service of emergency hyperbaric medicine that has been presented (already 10-15 years ago) in the corresponding special instructions on hyperbaric medicine.111 We believe that the data presented in this review may provide a justification for intensified research of hyperbaric therapy for blast/blunt injuries and for the creation and application for these purposes of mobile, multi-place hyperbaric chambers designed not only for military/field use, but, in today’s circumstances, also for inner-city use.181
ACKNOWLEDGEMENTS
The authors thank Ilia Stambler for editorial assistance and Dr. Efrat Barbiro-Michaely for help with the manuscript (both of Bar-Ilan University).
REFERENCES
Table 1. Characteristics of cardiorespiratory function in victims after severe blunt chest injury (mean + SD). Click on the table to open larger image in a separate window...
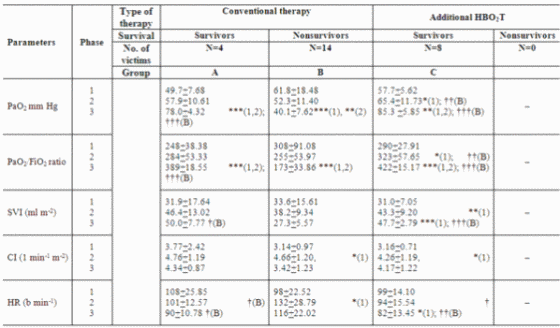
PaO2 = arterial partial pressure of oxygen; PaO2/FiO2 ratio = ratio of the partial pressure of arterial oxygen to the fraction of inspired 100% oxygen. SVI = stroke volume index; CI = cardiac index; HR = heart rate. See text for definitions of phases 1-3. This table shows statistically significant differences of mean values after comparison of all phases and groups. Values are shown as mean (SD). *Significant differences between phases, P<0.05; **Significant difference between phases, P<0.01; ***Significant difference between phases, P<0.001. The number inside the brackets beside symbols represents phase number. †Significant difference between Groups A (or C) and B, P<0.05; ††Significant difference between Groups A (or C) and B, P<0.01; †††Significant difference between Groups A (or C) and B, P<0.001.
Figure 1A.
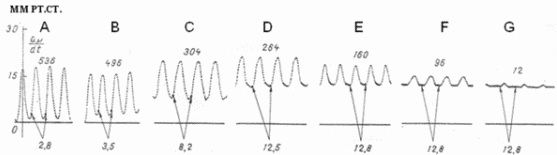
The dynamics of intraventricular pressure during respiratory distress syndrome (RDS) development in a dog model (A-G). Numbers above the curves represent the rate of change in the intra-ventricular pressure during diastole (mmHg), numbers beneath the curves show the absolute values of end diastolic pressure (EDP). Arrows indicate the moment of EDP measurement.
Figure 1B.
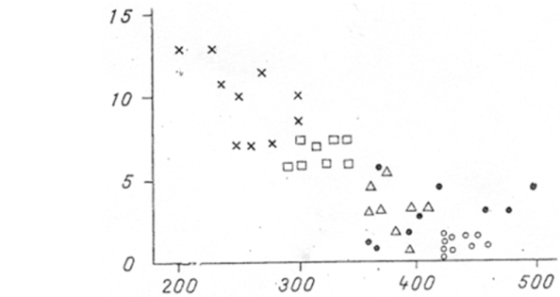
The relationship between end diastolic pressure (EDP) in the right ventricle and PaO2 in the end of 15 min oxygen inhalation in an experimental ARDS model. The X axis shows PaO2 (mmHg), the Y axis presents EDP (mmHg). Open circles – the initial state, full circles – the first stage, triangles – the second stage, squares – the third stage, crosses – the fourth (fatal) stage.
Figure 2.
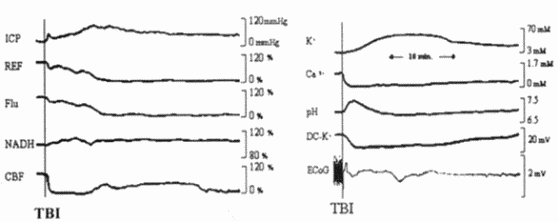
Analog responses of a rat exposed to severe injury. ICP – intracranial pressure; REF – reflectance; FLU – fluorescence; NADH – mitochondrial NADH redox state; CBF – cerebral blood flow; K+, Ca2+, pH – extracellular levels of ions; DC-K+ – DC potential for K+ electrode; ECoG – electrocorticogram.
Figure 3.
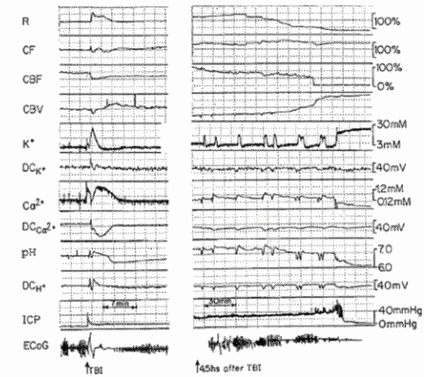
Multiparametric responses to severe head injury induced maximally in a rat from a severe group. The TBI led to a cortical spreading depression (CSD)-like response. The CBF decreased and reached a new steady state. CSD cycles and epileptic activity were recorded 4.5 h after TBI induction. The ICP level was elevated gradually until the final point, when the rat died and ICP dropped to 0. ICP, intracranial pressure; R, 366 nm reflectance; NADH corrected fluoroscence; CBF, CBV, cerebral blood flow and volume; K+, Ca2+, H+, extracellular concentrations of potassium, calcium and hydrogen ions; DCK+, DCCa2+, DCH+, DC steady potential measured concentric to the tree electrodes; ECoG, electrocorticogram.
Figure 4.
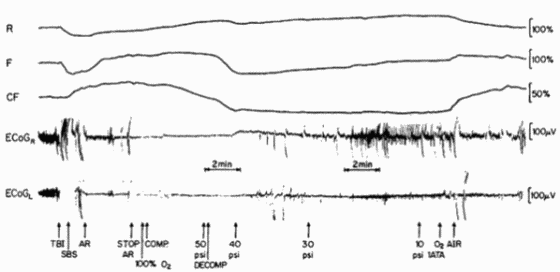
Metabolic and electrical responses in the rat brain before and after severe lateral fluid percussion treated by hyperbaric oxygenation. 'A' shows the effects of TBI (4.5-5 atm) and recovery by hyperbaric oxygenation: SBS -spontaneous breathing stopped; AR – artificial ventilation; stop AR – stop artificial ventilation; Comp – compression with 100% O2; Decomp – initial decompression; 50, 40, 10 psi – the level of compression O2 in chamber; Air – breathing of room air.
Figure 5.
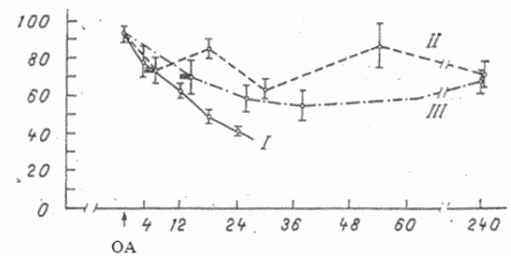
Dynamics of PaO2 after intrapulmonary injection of oleic acid (OA) (0.3 ml/100 g). Abscissa - time (hours); ordinate - PaO2 (ml Hg). I) Control series; II, III) series of experiments with HBO2 exposure, carried out 4 and 12 h after OA injection, respectively. Shaded rectangles indicate the period of HBO2 session. Arrow indicates the time of OA injection.










