TRCS - Transportable Hyperbaric Chambers For Emergency Evacuation And Treatment

Photo courtesy of Robert L. Sands
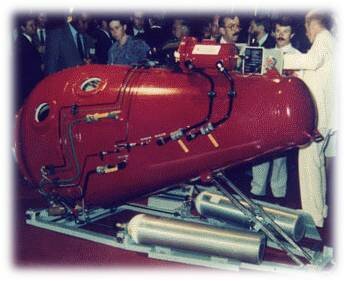
Among several types of transportable hyperbaric chambers this S-200 TRCS (Transportable Recompression Chamber System) is uniquely designed for emergency evacuation and treatment of decompression sickness, air embolisms, blast injuries, smoke inhalation in victims of accidents, disasters, terrorist acts or military operations.
The conical Transportable Recompression Chamber (TRCS) module and the Transfer Lock (TL) module feature the international NATO flange for a rapid transfer-under-pressure of casualties. The SANDS S-200 TRCS is manufactured in the United States to full ASME-PVHO-1 codes is in World-wide use. The chamber is designed for use in two modes:
- Hyperbaric Ambulance Mode: The TRC chamber can quickly transfer casualty from a disaster site to a bigger hospital chamber or emergency room.
- Hyperbaric Field Hospital Mode: By locking the conical TRC chamber to the cylindrical Transfer Lock, up to five patients can be treated.
Such portable hyperbaric oxygen chamber can be easily installed on any kind of transport craft - fixed wing, rotary blade, seacraft and road vehicles with low human resource requirement and major use of on-site available resources. With practice, trained personnel could set up a HBOT MASH (Mobile Army Surgical Hospital) system in less than 30 minutes.
Pacific Ocean (July 16, 2004) -- Gunner's Mate 1st Class (DV/SW) and Sonar Technician Surface 3rd Class (DV)Jeff Griggs, Navy Divers assigned to Mobile Diving Salvage Unit One, perform pre-diving operation procedures on the Transportable Recompression Chamber System during mixed gas diving salvage operations in support of exercise Rim of the Pacific (RIMPAC) 2004. RIMPAC is the largest international maritime exercise in the waters around the Hawaiian Islands.

Photo courtesy of "Slagheap"
Today there is a real need for such mobile rescue capsules in the world. Often there are significant deficiencies in providing a more efficient life support means while transporting casualties from a disaster sites.

Robert L. Sands, the designer and patent holder of this unique Transportable Recompression Chamber System, worked with many worlds foremost hyperbaric research facilities and also with the U.S. Navy on a collaboration basis. In 1990, Robert Sands was described as one of the worlds "foremost diving and hyperbaric engineering designers . . . with considerable interpersonal skills, enthusiasm and vision". He is a founding member of the International Hyperbaric Medical Association and continues to be a top pioneer in his field today. Robert L. Sands is C.E.O. and Founder of Healing Chambers International, Inc.
Administrator of this website is indebted to Robert L. Sands who kindly permitted to publish quotes from our correspondence and his feedback on recently published article on the topic of blast injuries and HBOT. The inevitable question was rised during our exchange, which follows
"Why a much wider deployment of TRC Systems is still not a mandatory rescue measure in major disaster sites like massive fires, blasts, battle fields, etc..?"

The day after September 11, WTC. Count the heroic souls that are breathing from compressed air breathing apparatus (BA) and those that are not. HBOT should at the site -- plenty of TRCS. Did not happen.
"The only time the U.S. Navy has used their TRCS for civilian use was at the Quecreek Mining accident in 2002.
7/26/2002 12:00 PM - The U.S. Navy has joined the effort to rescue the nine trapped miners. The Navy has sent underwater medical experts and nine portable hyperbaric chambers to the scene. Decompression will be necessary when the miners are rescued. The allowance was made because it was feared that the miners were suffering decompression sickness.
It is likely that most of the rescued nine were suffering some form of DCS, however the protocol to ride in the TRCS required all rescued personnel to be showered to remove any dirt or coal dust in case this "caused an explosion" within the chamber. It is believed that more than 40 USN personnel accompanied the nine TRC rescue capsules along with tons of ancillary equipment. "
"...sometimes it is easier to obtain forgiveness than get permission..."
"...I spent a lot of my life - about ten years and my youth and a marriage - and one of the big chunks of money on arriving at the correct design of the Transportable Recompression Chamber (TRCS) that the US Navy has more than sixty in fleet use. My original design envelope was that the two pieces should be deployed in the old Bell UH series ("Huey") helicopter, and that sufficient room be available in the tiny cramped cabin needed to allow for a one-hour in flight with treatment under pressure.
The TRCS S-200 design calls for them to be built like a hockey puck and I designed redundancy factors galore . . . "if Alpha circuit fails, use Bravo. If Both fail, there is always Charlie system." I had in mind that all you needed during transport was adequate oxygen for the BIBs and a couple of SCUBA tanks and a small air compressor to charge on of them during flight. There is a large amount of 12 - 24 v power easily tapped on all transport craft (fixed wing, rotary blade, seacraft and road vehicles.)"
About Sands Chambers. The company had its roots down under and the introduction of Sands chamber designs came about by a curious occurrence. In the early 1980's Sands was designing an inflatable portable chamber system. The Australian Government's Department of Industry and Science appointed Sands to research and develop a transportable chamber. The trigger factor was the discovery and archaeological excavation of the Royal Navy Frigate, HMS Pandora.
Sands discontinued R&D on the inflatable chambers because they were scientifically unsound. Instead, he concentrated on a two piece, double lock 6 ATA transportable chamber system (TRCS) that was robust and met with standards of both hyperbaric and diving physicians. The Sands TRCS design is now in fleet wide use by the US Navy, Coast Guard and the Marine Corps as well as fire and rescue services around the world. In 1990 Sands relocated to San Diego.
The impetus was Dr. Nuebauer who asked him to design chambers for traumatic brain injured patients. Since many of these patients have contractual deformities the Sands III is the largest monoplace (48 inches) in the world. For the past 15 years the chamber has set the standard for ease of accessibility with its unique comfort couch. The latest design is collaboration with ICHM specialist physicians. Known as the Sands VII, it will be released soon.
"Give you two instances, other than blast. 911. The US DOD should have had a huge parking lot full of them for the rescue workers and they should have been working around the clock for a month. Did not happen.
A couple of years back, huge wildfires surrounded San Diego. It was just like Armageddon is imagined. 13,000 firefighters on the line and two thousand homes lost. Again, no TRCS. In fact, since all of the big hospitals have to "make air" from outside, the smoke and particles meant that all of the San Diego multiplace hospital chambers closed of operations during that critical time. My center in San Diego was the only one available to treat fire fighters that were smoked. 24/7 during the week of the emergency.
Then, two years later, it happened all over again. This time I contacted every person in the USN that I know. Still, the TRCS were kept hidden away. "
"In 2004 we delivered chambers to the Fire and Rescue Department of Malaysia (FRDM) and spent about 3 months in training layers of them. If you follow the numbers on the picture u will see that there are three layers.
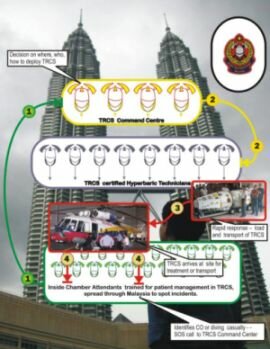
The first responders (bottom level) were taught how to recognize a problem and then stay with the casualties until the TRCS arrived. These first responders were the inside attendants who would stay with the patient during treatment and or transport. They would then call in to the top level in FRDM commanders who would make GO/NOGO decisions and transport asset decisions.
They would then talk to the middle level, and two on duty chamber operators would accompany the TRCS to the accident/trauma site and treat the patients plus the trained inside TRCS attendant. Low human resource requirement and major use of on-site available resources. With practice, the FRDM personnel could set up a HBOT MASH system in less than 30 minutes.
When I trained the Malaysian Rescue Service in the use of the TRCS, I had it so they could operated these Portable Hyperbaric Chambers on a tank of oxygen and use their fire-fighters breathing apparatus ("BA"). Every fire department around the world use BA and have BIG compressors to refill them at the site of a major blaze. Why not a truck with TRCS on board? And, there was plenty of room for transports under pressure in their big Russian "BOMBA" choppers.

What is more, I designed the TRCS to be operated on air press-down, with O2 on BIBS, or to bypass the BIBS by pressing down on 100% O2. The way, in the event of a fire or bio warfare problem, you could stack at least 3 casualties (or more) plus a medic into the coupled TRCS. The Malays quickly adopted that protocol. And just two folks to operate the chambers and just a small amount of ancillary equipment."
"...soft tissue damage and edema was one of the major control problems at the Iraq and Afghanistan MASH units..."
"My sister-in-law is a full bird USF Colonel Flight Surgeon. Up until a year ago, she was the head specialist MD at one of the USAF Hospitals in Europe. Get shot or wounded in Iraq, and six hours later the casualty was landed at her hospital and it was her team that took over the emergency surgical care.

Photo courtesy of "tattooed_4life"
One of the big questions she had for me stemmed from her comment that all casualties had immense soft tissue damage -- edema beyond anything she had ever seen. And this soft tissue damage was one of the major control problems her team had in trying to save the casualties life or reduce the damage so there would be a better chance of rehabilitation and a normalized life when they were out of uniform.
It seems that at the Iraq and Afghanistan MASH units, there is a rush to stabilize the patient to get them on the flight to Europe. Amputations and colostomies were common. There was a need to get these patients out of the desert dust. I then pointed out something to my sister-in-law during her visit to San Diego."
"Have you noticed that when you fly back to the US from Europe, your feet swell? The reason is that for your nine hour flight you are breathing 17.6% O2 when the aircraft is at cruising altitude of 38,000 feet. This means that there is a hypoxia affecting all body cells.
The most evident effect is that endothelial cells hold a lot of nitric oxide. When hypoxia sets in, the endothelial cells, particularly those on the venous side of the circulatory system suck in a lot of water from plasma and interstitial fluid.
Keep in mind here that not only is there hypoxia during flight, there is a decompression sickness problem as well. The body contains approximately 3% body-weight of Nitrogen (N) in chemical form at sea level. A rough calculation is a 200 lb. (90 Kg.) man will have 6 lbs (2.7 liters). of N inside him as a liquid.
During flight, Dalton's Law kicks in and the N disassociates. Without getting too technical and not knowing the speed of the off gassing of the N, it is likely that the patient bleeds off near on a liter of N. There is no compensatory effect of breathing 100% oxygen as there is in a HBOT chamber during the flight.
According to a very clever American HBOT specialist, Keith Van Meter, M.D., all jet lag after a long flight is enhanced by the passenger/patient's of sub-clinical DCS. (That is why a ride in a chamber after a long flight will "set your clock right.") According to Van Meter, a ride in a chamber after landing should be mandatory for all flight crews."
"Jumping sideways a tad . . . one of the extremely bright specialists on the HCI Scientific Board is a USN research physician in San Diego Beatrice Alexandra Golomb, MD, PhD, pointed out to me that she always has supplemental oxygen on all long overseas flights "I am the only one of the group that hits the ground, bright and perky." I might add, Beatrice is formidably fit. She also pointed out that strokes and heart attacks are common on long flights "because the mitochondria are so insulted by hypoxia in an older person, or a person with underlying health problems." Because of her comments and thoughts we always strongly advise our cancer patients NOT to fly and if they have to, do so with supplemental oxygen.
Back to transporting blast injuries. During transport, the dynamics of physics and physiology really kick in. Plus the fact that the casualty is usually on a plasma expander to keep blood pressure up, bleeding or not. All of that extra fluid has to go somewhere. NO swelling with H2O in endothelial cells. And it is even worse for those with closed head injuries (these signature injuries with hydrocephalus making their post traumatic stress disorder more likely to stick. Steroids are not the answer but are used, along with carbon dioxide inhalation. For swollen brain. Fastest and safest way to reduce ICP is HBOT."
So, what is the answer with blast injury casualties?
"...To use a chamber during a six hour flight? No, Only to use in the retrieval of a DCS or CAGE patient during rapid and fast transport to a bigger HBOT facility for repeated treatments. Or, depending on the call of the flight surgeon, to press the patient down during the flight for 60 minutes. Certainly, the little 1,300 lb conical rescue chamber of the two-part TRCS would no take up much space on a big USAF transport aircraft.
Certainly, if I had my way, I would use HBOT after the patient was stabilized. Either pre-transport or post-transport or both. And, in an emergency, during transport. The way it was designed to operate. And again, if I had my way, I would shake all of these chambers loose for civilian use. The cost of 911 rehab of rescuers, workers and victims would now be a fraction and many of the hundreds that later died from bio-hazard inhalation would still be with their families."

Photo courtesy of Robert L. Sands
Return from the Portable Hyperbaric Chambers TRCS overview to the Home Page











